













Case Presentation:
Acoustic Neuroma - Case 1
History & Physical
- 49-year-old left-handed gentleman who had undergone subtotal resection of a right vestibular schwannoma (acoustic neuroma) nine years ago at a different institution followed with stereotactic radiosurgery. After that operation, he had experienced a complete loss of hearing on the right side, right facial weakness, and difficulty with balance and gait all of which had improved post operatively.. He was followed radiographically since. Recent radiographic studies revealed enlargement of the tumor, and the patient presented to us for assessment and treatment planning of his tumor growth despite surgery and radiosurgery at a different institution.
- On physical examination, he had House-Brackman Grade III facial weakness on the right, and no hearing on the right.
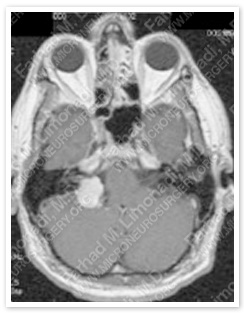
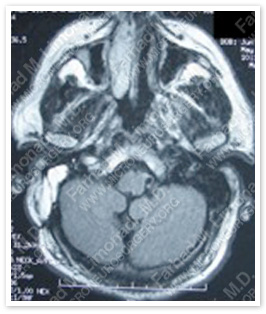
Imaging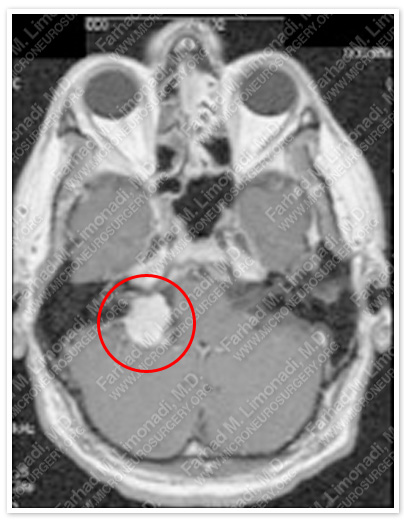
MRI scan of patient’s brain shows a recurrent large right acoustic neuroma
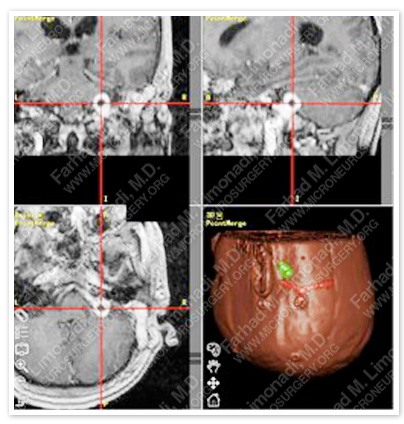
Computer navigation is used to pin point the location of tumor. Tumor is shown in green in the right lower picture and is under the hairpin on MRIs.
Surgical Procedure:
- He underwent a redo translabyrinthine resection of this tumor using computer navigation and stereotaxy and intraoperative neurophysiological monitoring including facial nerve monitoring and brain stem auditory evoked response (BAER).
Pathology:
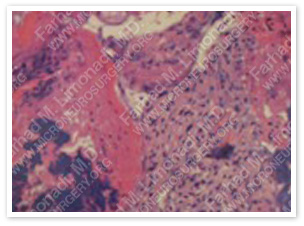
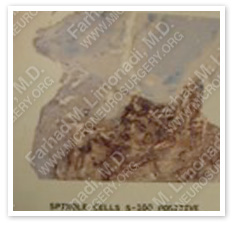
The pathology of the tumor confirmed diagnosis of acoustic neuroma (vestibular schwannoma).
Post-Op Imaging:
Before Operation After Operation
Post op MRI confirms complete resection of the tumor with no injury to surrounding neurovascular structures.
Post-Op Course:
- The patient did well postoperatively despite the complexity of the operation due to being a redo, as well as radiation therapy. He was discharged home and has returned to full-time employment. His right facial paresis initially was worse than preoperative time; however, over the course of time his facial weakness improved significantly and returned to his base line (House-Brackmann Grade III).