













Case Presentation:
Spinal Cord Tumor Neurofibroma - Case 3
History & Physical
- 69 year-old lady with 5 years history of numbness and tingling of arms and legs attributed to peripheral neuropathy, who presents to the emergency room with weakness of upper and lower extremities, and bowel and bladder incontinence of a few weeks duration.
- On physical examination, patient has upper tract signs with mild weakness of upper and lower extremities.
Imaging
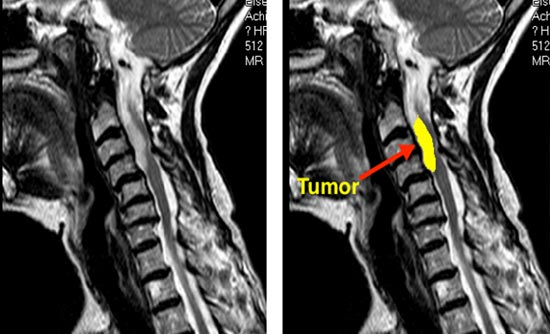
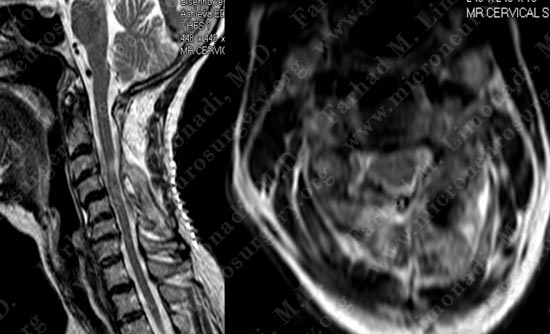
MRI scan of her cervical spine (neck) shows a large intra-dural, extra-medullary tumor pressing on the spinal cord at C2-C4 level and causing significant spinal cord compression. The tumor is marked on the right slide which is a sagittal view of the cervical spine.
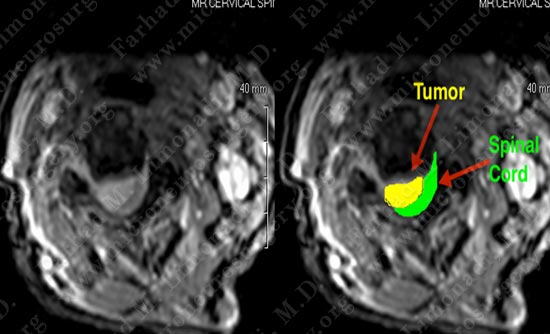
MRI scan of her cervical spine (neck) shows a large intra-dural, extra-medullary tumor pressing on the spinal cord and causing significant spinal cord compression. The tumor is marked on the right slide which is an axial view of the cervical spine.
Treatment Plan
- Patient was indicated for surgical resection of the tumor.
- Given the location of the tumor the plan was made to proceed with a posterior approach consisted of wide laminectomy, right sided facetectomy, and a lateral and posterior approach to the tumor, followed by lateral mass screw fixation to avoid spinal column instability.
Surgical Procedure
- She underwent C3-C4 and partial C2 laminectomy, C3 and C4 right sided facetectomy with exposure of the dura (covering of the spinal cord).
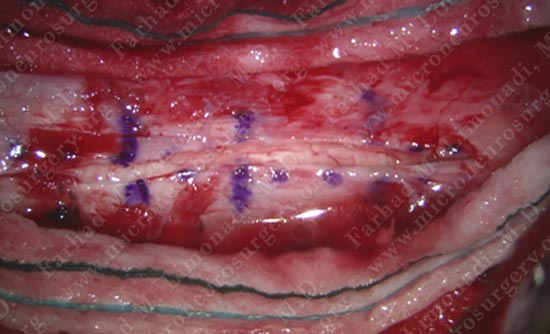
Dura is shown above with the planned incision site which is slightly off center, marked with a blue pen.
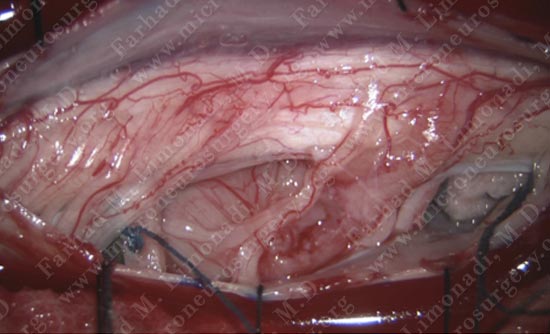
Dura is opened carefully and the underlying spinal cord well exposed. The tumor is readily visible pushing the dura posteriorly on to the left side of the spinal column.
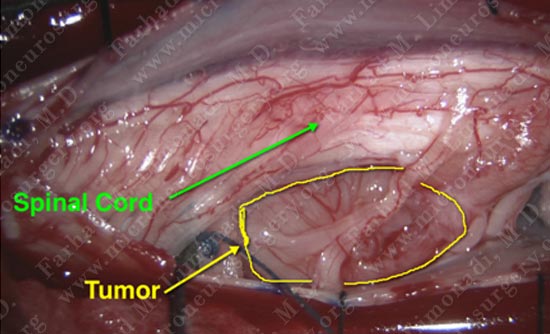 Tumor and spinal cord are both marked above.
Tumor and spinal cord are both marked above.

Higher power magnification with the tumor readily visible pressing on the spinal cord.
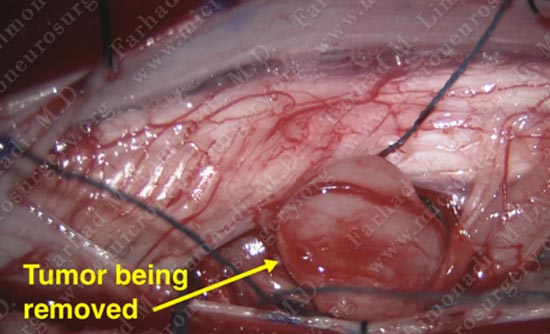
While patient is being electro-physiologically monitored with intra-operative spinal cord stimulation, the tumor is carefully removed utilizing microsurgical approach. Tumor and spinal cord are both marked above.

Spinal cord is free from compression by the tumor after complete resection of the tumor. It is carefully mobilized to the center of the spinal column to prevent tethering of the cord.
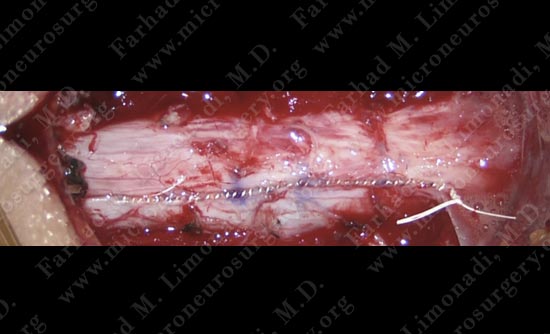
Dura (covering of the spinal cord) is carefully micro-sutured.
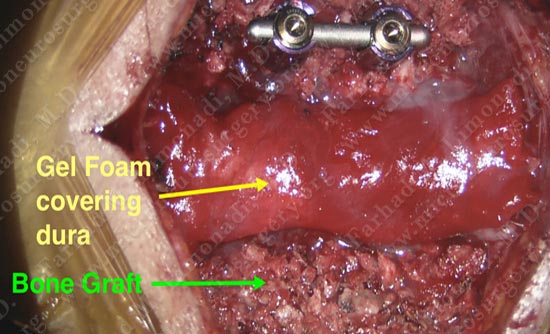
Instrumentation is completed on the left (top of picture), with bone graft placed on the lateral masses on both sides and dura protected with gel foam.
Post-op Imaging
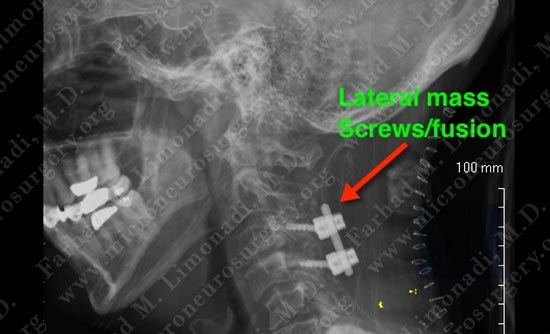
X-ray shows excellent position of instrumentation.
Post-op Imaging
X-ray shows excellent position of instrumentation.
Post operative MRI shows complete resection of tumor.

Post operative MRI shows complete resection of tumor.
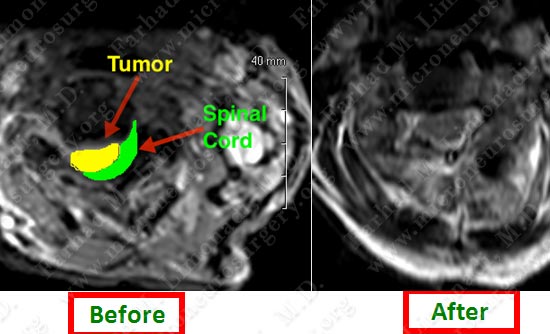
Post operative MRI shows complete resection of tumor.
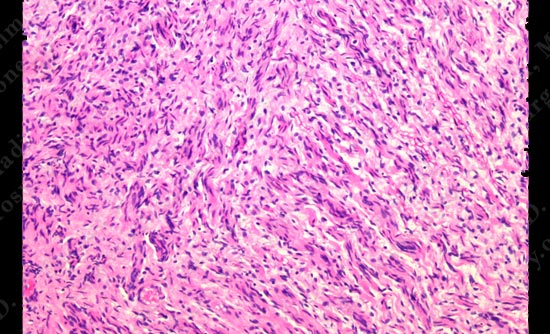
Pathology of the tumor was that of a spinal neurofibroma. Additional work up ruled of Neurofibromatosis type 1 or 2.
Post-op Course
- Patient did well post-operatively with no new neurological deficit. Her bowel and bladder function returned to normal.
- She was discharged home and returned to regular function and remained tumor free.