













Case Presentation:
ACOM Aneurysm - Case 4
Anterior Communicating Artery Aneurysm
History & Physical
- 70+ year-old lady who presented to the emergency room with the worst headache of her life as well as neck pain.
- On physical examination she was awake, alert, and oriented lady who had significant photophobia, and meningismus (spasm of the neck muscles).
Radiographic Studies
 CT scan of her brain demonstrated widespread subarachnoid hemorrhage. On the right slide
CT scan of her brain demonstrated widespread subarachnoid hemorrhage. On the right slide
Subarachnoid hemorrhage is outlined in red marking.

Cerebral angiography demonstrated an ACOM (anterior communicating artery) Aneurysm. On the right slide the aneurysm is outlined in yellow. She has a dominant left A1.
Treatment Plan
- Due to complexity of the morphology of the aneurysm, with wide neck, and branching vessels arising near its dome it was not considered safe for interventional approach.
- She was therefore, prepared for a left sided supraorbital approach for micro-clipping of the aneurysm.
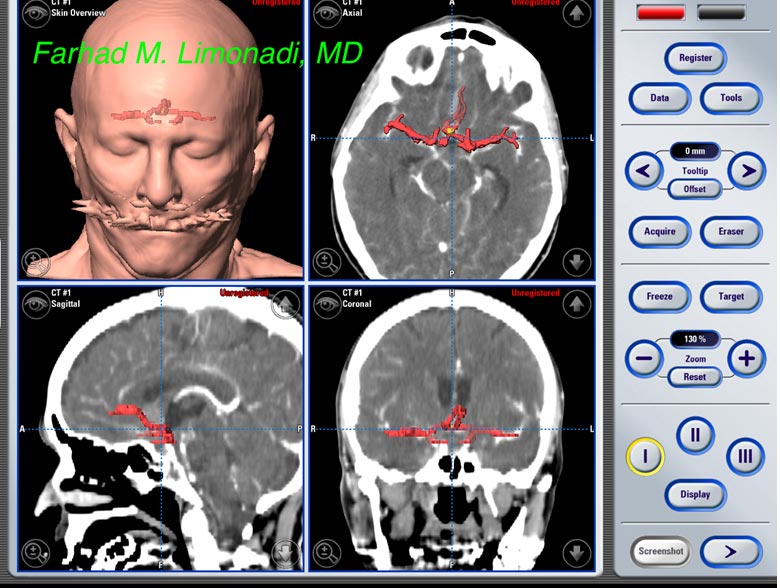
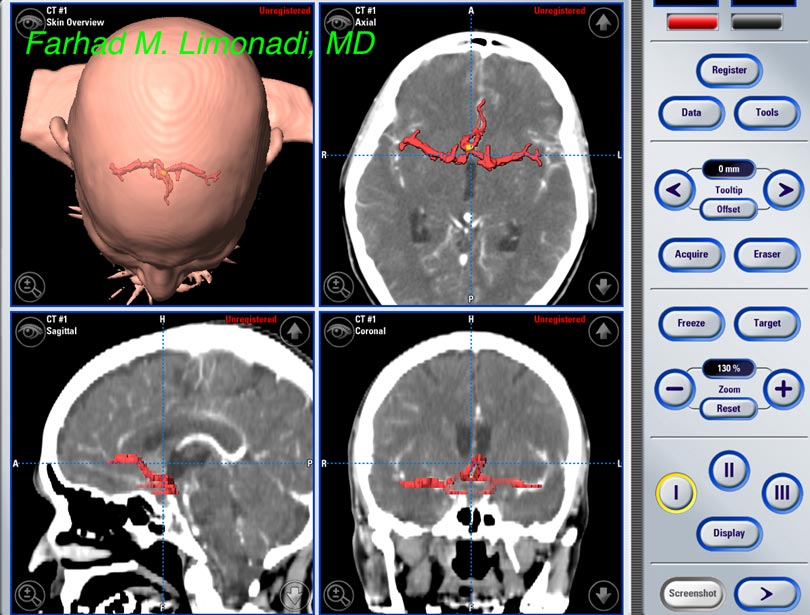
- Computer navigation and stereotaxy and intra-operative neurophysiological monitoring was utilized during the approach.
Operating Room
- Computer navigation/ stereotaxy was utilized to locate the aneurysm with pinpoint accuracy and its borders with surrounding structures were studied using 3D modeling.

Surgical Procedure

A small supraorbital craniotomy of approximately 1 inch has been performed.
(view through the surgical microscope)
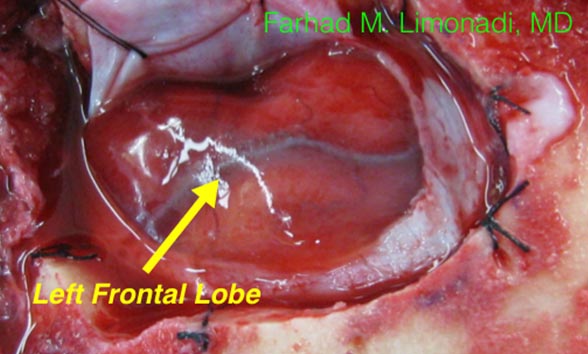
Dura is opened and left frontal lobe is nicely exposed. Please note blood in the subarachnoid space which is typically not seen in other cases.
(Magnified view through the surgical microscope)
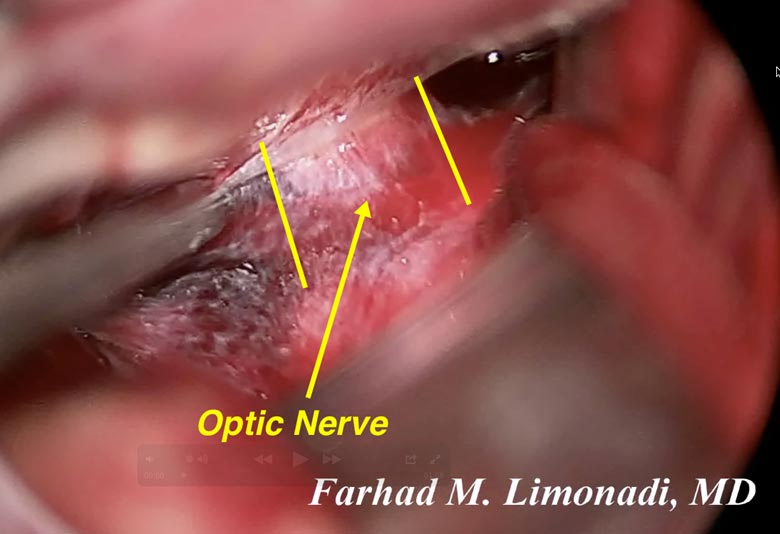
Upon gentle retraction of the frontal lobe, optic nerve covered by arachnoids and blood is visualized. This veil of arachnoid is carefully incised to expose the optic nerve and carotid artery.
(Magnified view through the surgical microscope)
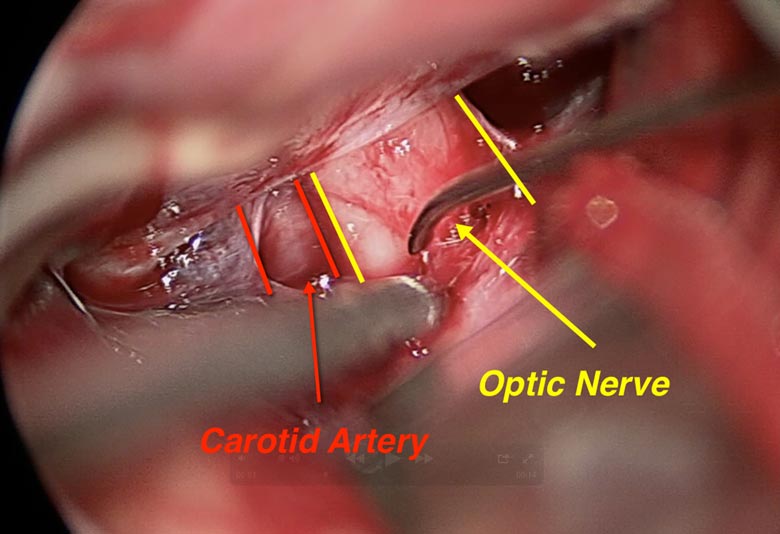
Optic nerve and carotid artery are nicely exposed.
(Magnified view through the surgical microscope)
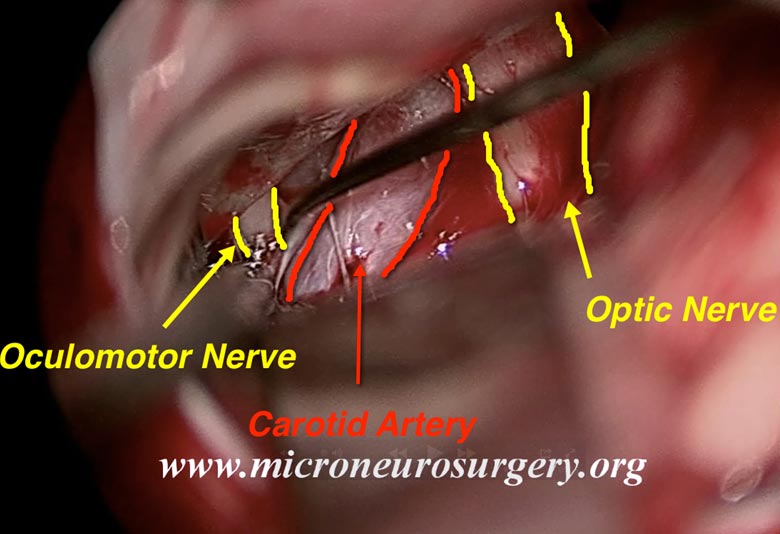
Oculomotor nerve (third cranial nerve) is also exposed.
(Magnified view through the surgical microscope)
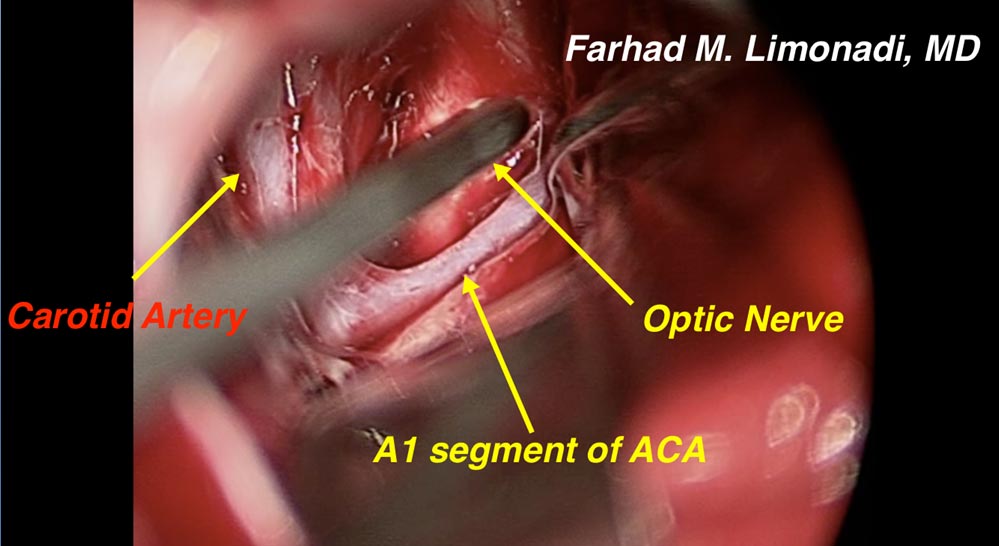
Dissection is carried medially along the course of first segment of anterior communicating artery (A1) to ACOM and finally the neck of the aneurysm.
(Magnified view through the surgical microscope)
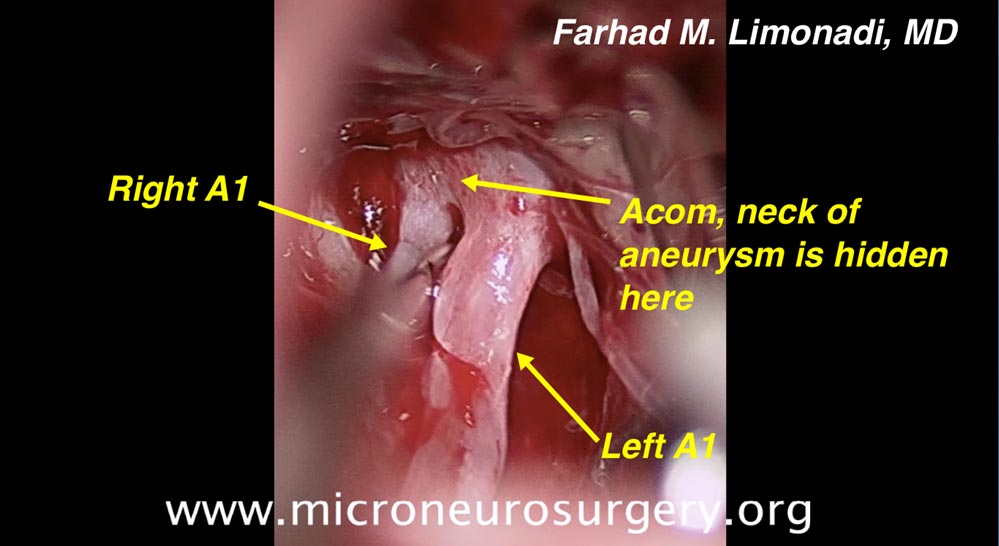
Left and Right A1, Acom, and the neck of the aneurysm is nicely exposed.
(Magnified view through the surgical microscope)
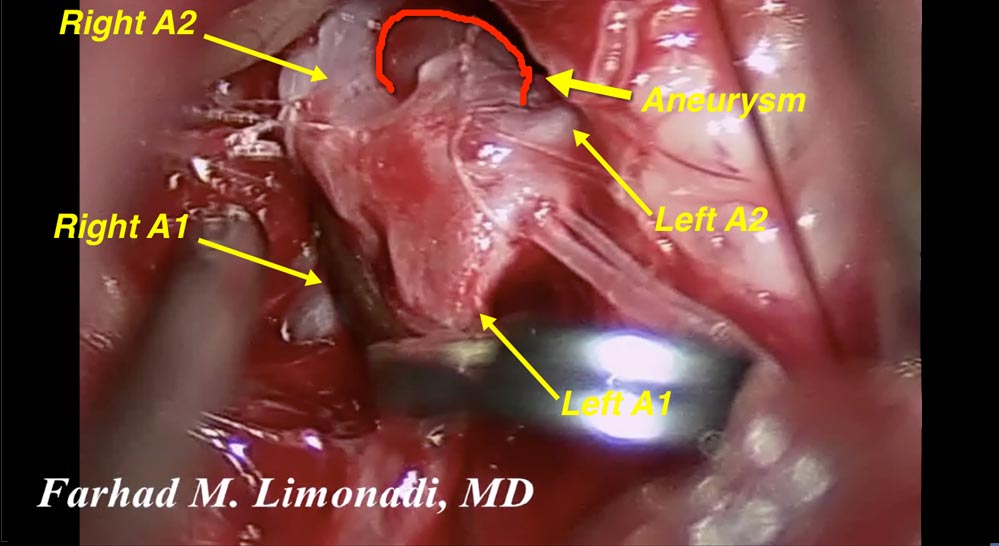
Left and Right A1, A2, Acom, the neck, and the dome of the aneurysm are nicely exposed. A temporary clip is placed to occlude both A1 during dissection of the neck and the dome of the aneurysm.
(Magnified view through the surgical microscope)
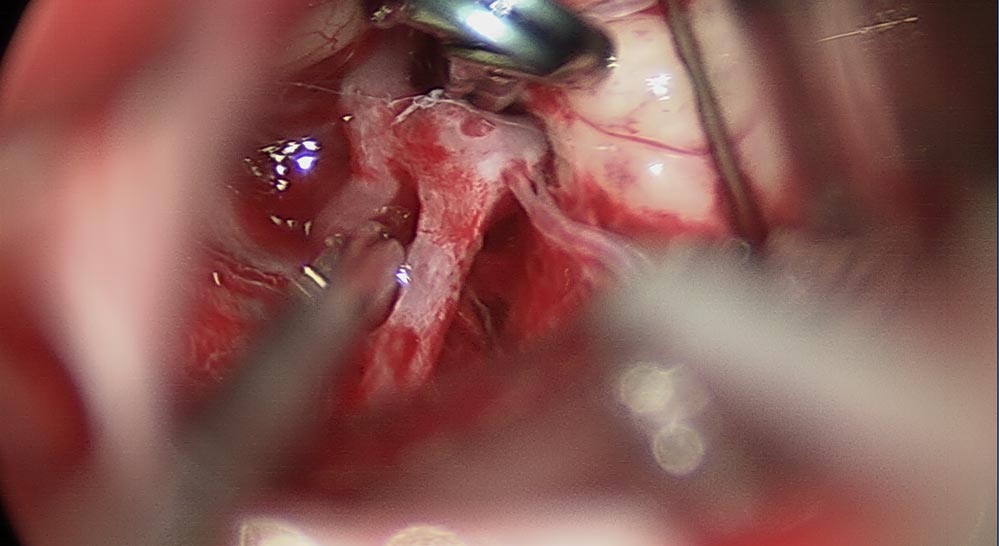
A titanium clip is placed around the neck of the aneurysm, and therefore, has eliminated it as a threat. The temporary clip has also been removed.
(Magnified view through the surgical microscope)
Video of Operation
Post ooperative Images
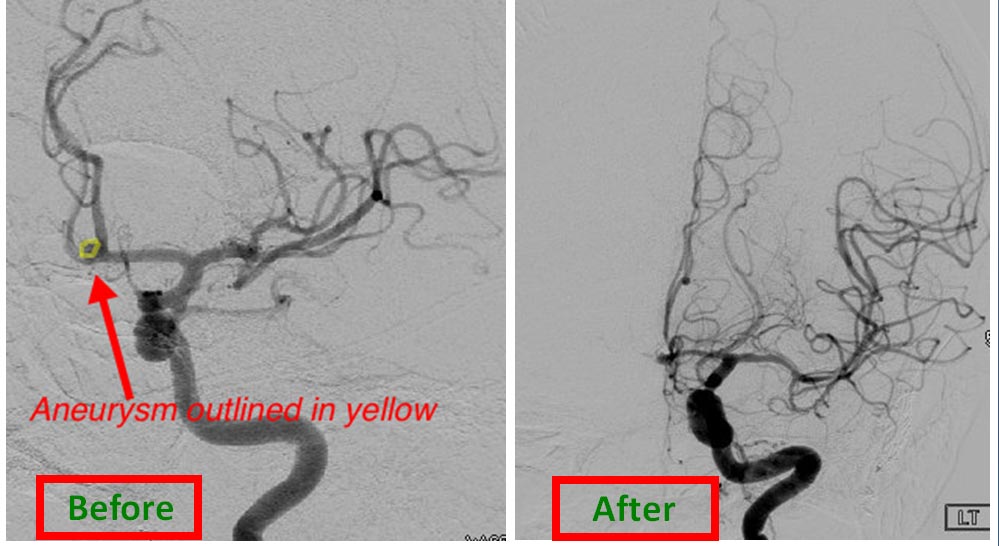
Post operative cerebral angiography confirmed successful elimination of the aneurysm.
She was discharge from the hospital and returned to normal function.