













Brain Stem Tumors - Case 2
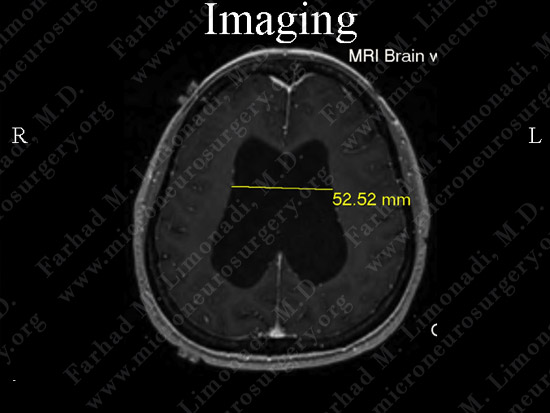
Brain Stem Glioma and Hydrocephalus
History & Physical:
-
36-year-old lady with a one-year history of hypertension, headache, and nausea and vomiting. After losing consciousness a couple of times, she was sent for radiographic study of her brain.
-
On examination, she exhibited upper tract signs, papilledema, and diplopia.
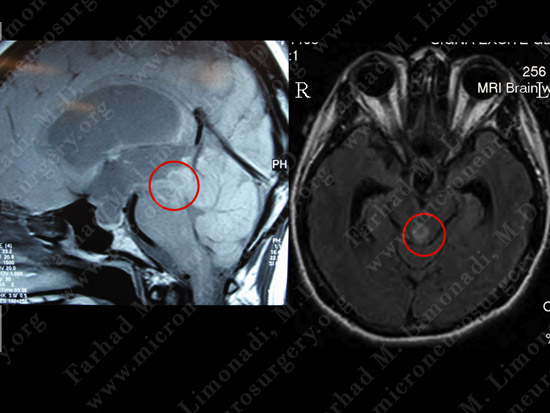
Imaging
Surgical Procedure
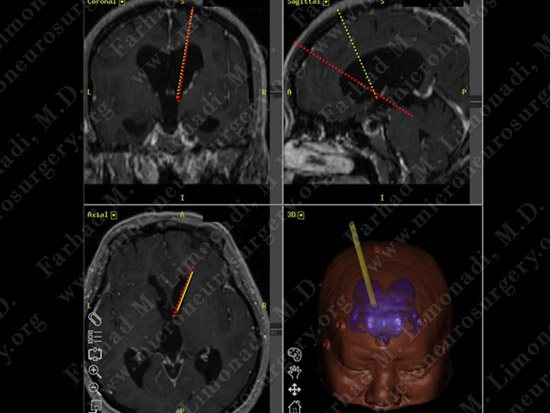
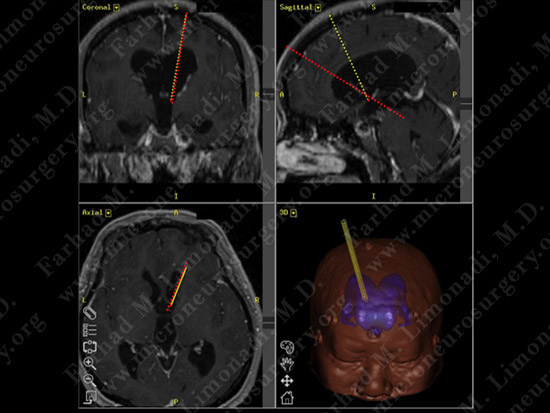
Computer assisted simulation was utilized to plan two approaches: red dotted line is the trajectory to the tumor, and the yellow dotted line is to the floor of the third ventricle for third ventriculostomy.
After induction of general anesthesia, the patient's brain and skull coordinates are co-registered to computer navigation system for the purpose of stereotaxy.

Dr. Limonadi and his team proceed with the third ventriculostomy using a small opening (dime size) in the skull. This procedure treats hydrocephalus as opposed to placing a shunt system.

During this step, the left monitor shows the actual surgical field through the small lens of the endoscope and the right monitor shows the computer navigation which functions as the radar system of the brain.
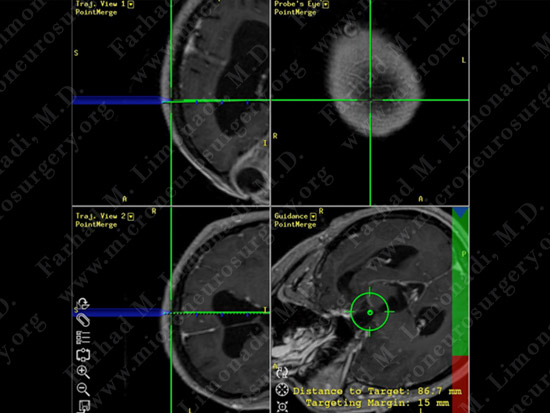
The monitor shows the endoscope (blue) resting on the small opening of the skull and aimed at the target (floor of the third ventricle). The right lower image shows the target and the distance.
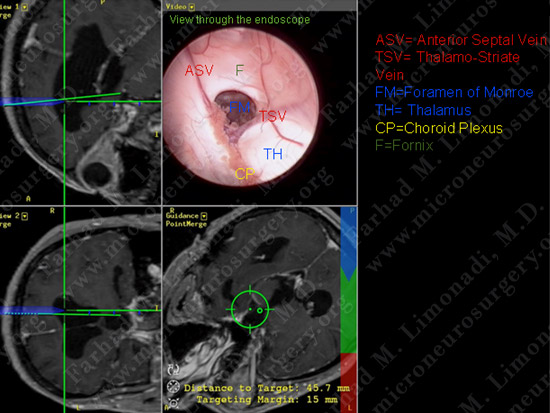
The monitor shows the endoscope (blue) entering the lateral ventricle and the surgical view through the small lens of the endoscope (right upper image) shows the anatomy of the lateral ventricle.
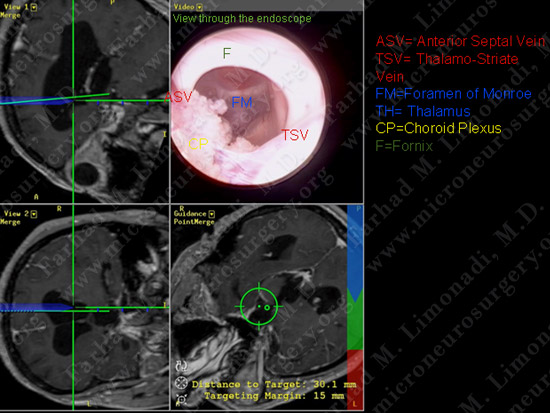
The monitor shows the endoscope (blue) entering the third ventricle through the foramen of Monro.
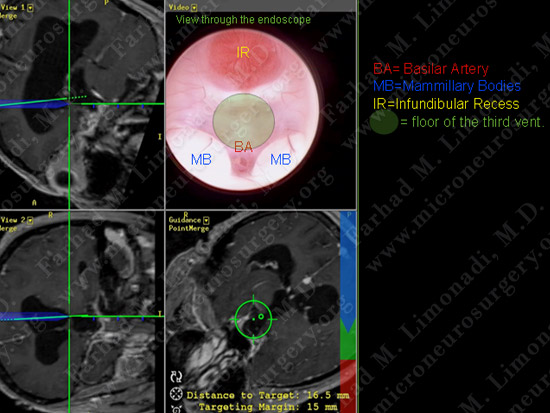
Third ventricle is entered and its anatomy is studied. The floor of the third ventricle is thinned out due to hydrocephalus and a stoma will be created here to complete third ventriculostomy
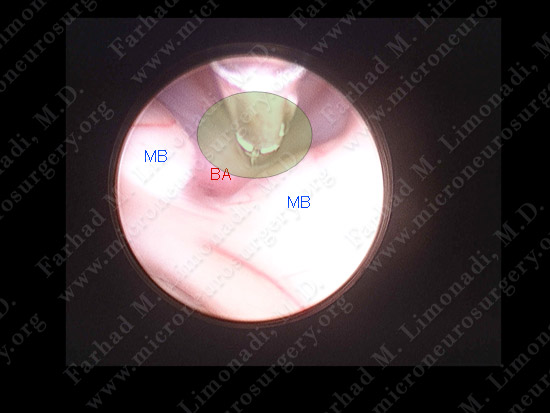
A micro-instrument is inserted through the working channel of the endoscope and used to create a stoma and the third ventriculostomy has been performed without complication. This successful operation averts the need for surgical implantation of a permanent ventriculo-peritoneal shunt in this patient.
Subsequently, through another dime size burr hole the red trajectory is utilized to approach the tumor.
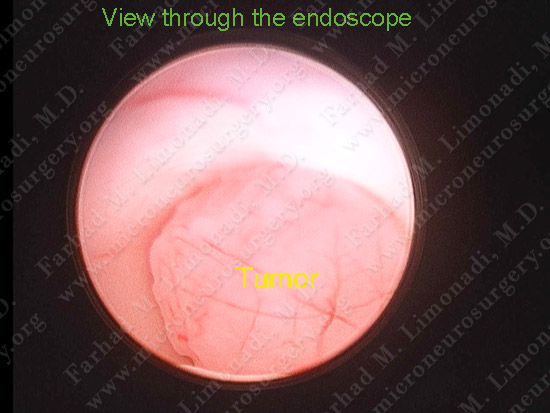
The tumor is found arising from the tectal plate of the midbrain and obstructing the aqueduct.
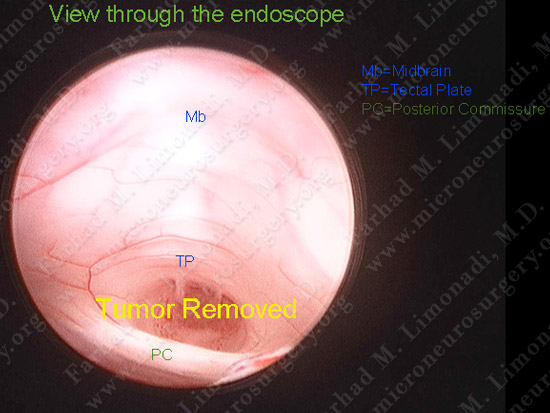
The tumor is removed through the small aperture of the neuroendoscope and the aqueduct is opened.
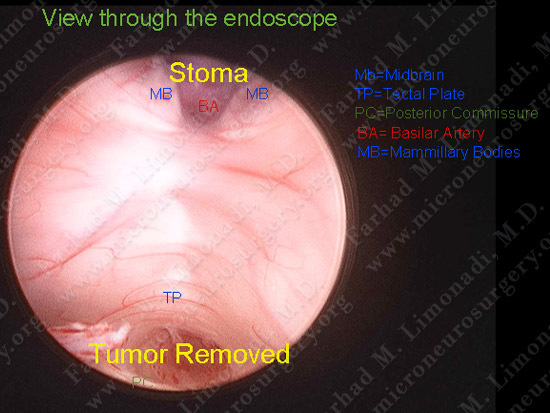
This single view through the endoscope demonstrates successful completion of both the third ventriculostomy and resection of the tumor.
Pathology
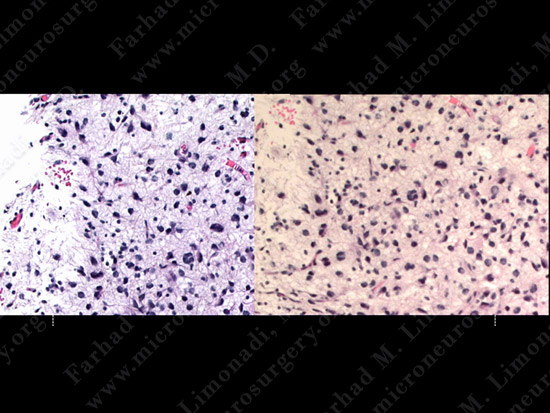
The pathology of the tumor confirmed diagnosis of anaplastic astrocytoma.
Post-op Course
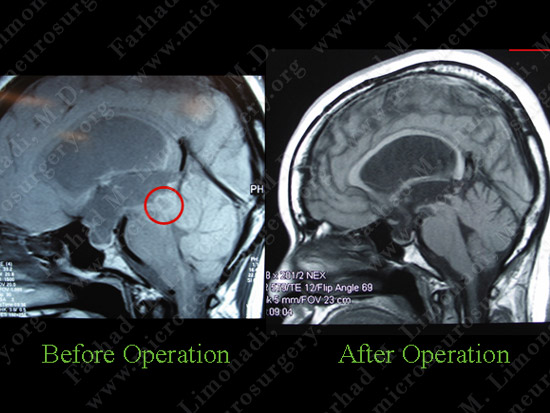
Post-op MRI shows complete resection of the tumor radiographically.
Post-op Course
Patient was discharged home with no neurological deficit. Here she shows her small incision.