







Case Presentation:
Colloid Cyst - Case 2
History & Physical
- 54-year-old lady with several episodes of syncope (sudden loss of consciousness) with possible cardiac sources of syncope ruled out.
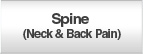
- CT scan of her brain revealed a colloid cyst in the roof of the third ventricle.
- On examination she had no focal neurological deficit.
- Patient was advised to undergoe endoscopic exploration and resection of the colloid cyst, however, she chose conservative measures with radiographic follow-up.
- After having two episodes of loss of consciousness (syncope) she was brought to Eisenhower Medical Center for evaluation.
Imaging
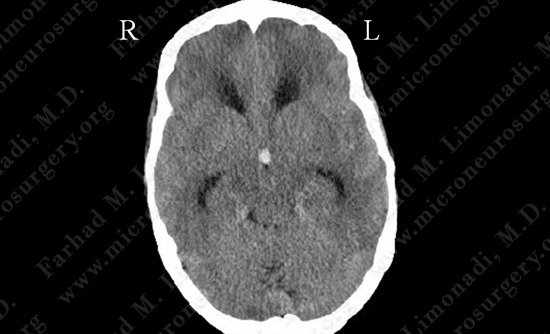
CT scan of her brain shows a colloid cyst crowding a small third ventricle and obstructive hydrocephalus with cerebral edema.
Surgical Procedure
- Given the small and crowded third ventricle with significant cerebral edema, minimally invasive approach of neuro-endoscopic resection of the colloid cyst was determined to be technically challenging.
- However, the decision was made to proceed with this approach and interhemispheric-transcallosal craniotomy (open surgery) reserved as a back-up.
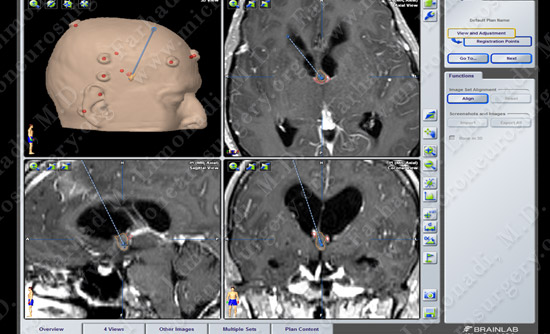
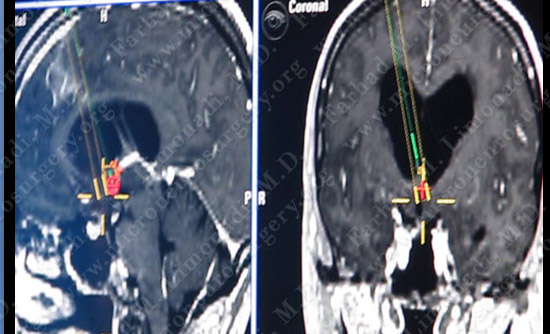
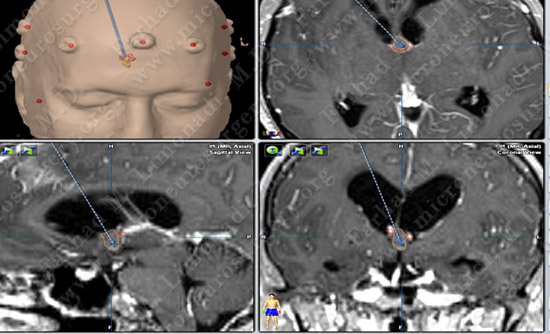
Computer navigation and stereotaxy was utilized to map and localize the Colloid Cyst. (outlined in yellow) during surgery.

Intra-operative neurophysiological monitoring including Brainstem Auditory Evoked Response (BAER), SSEP and MEP is utilized to monitor her brain functions during the surgery.

A larger area than normal is shaved in case we have to convert the surgery to open (interhemispheric transcallosal craniotomy).
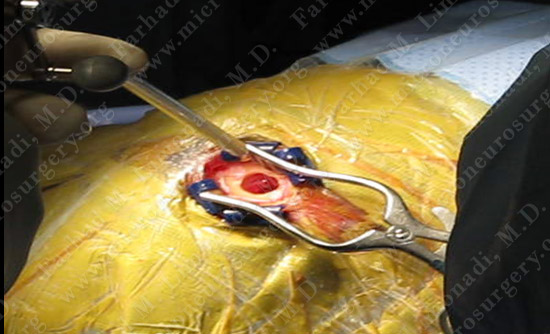
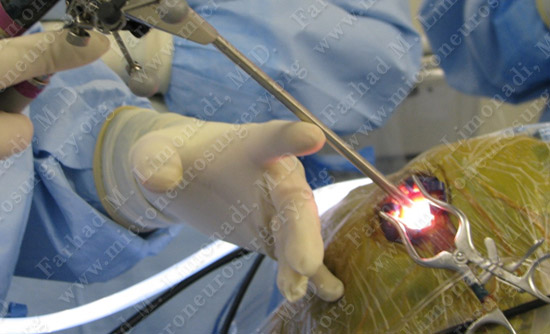
Neuro-endoscope is armed with stereotaxy, and using an incision of approximately 1 inch and burr hole (bone opening) with diameter that is smaller than a dime, the endoscope is driven to target using computer navigation and anatomical landmarks.
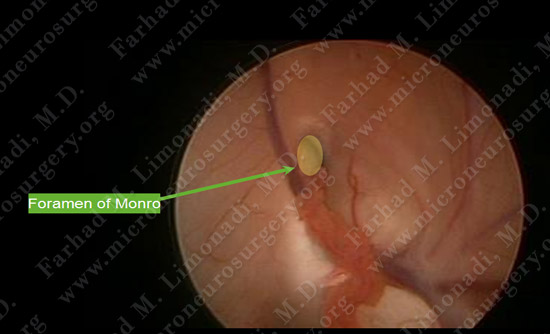
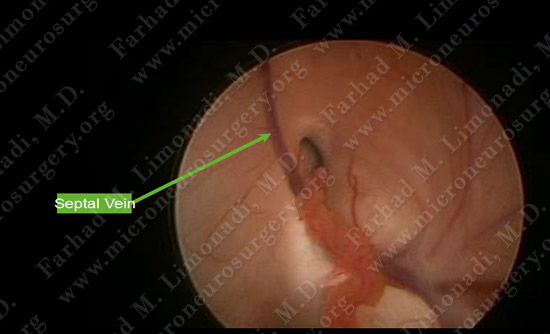
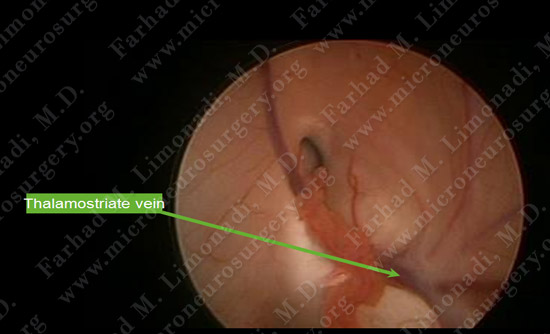
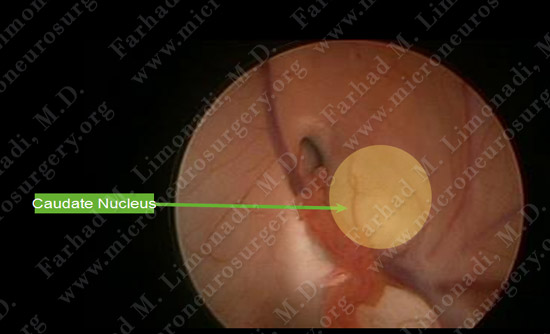
Upon entry into the frontal horn of the right lateral ventricle, import landmarks are identified.
Foramen of Monroe is found to be rather small increasing the technical difficulty of the case.
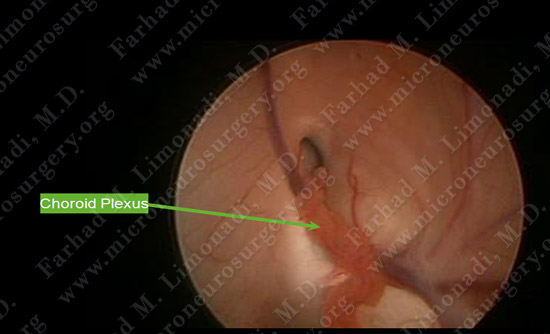
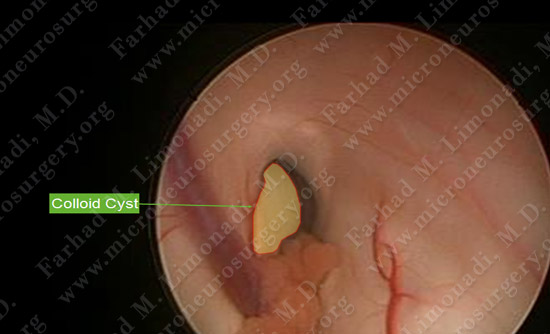
As then neuro-endoscope is driven closer to the forman of Monro, the colloid cyst becomes readily visible.
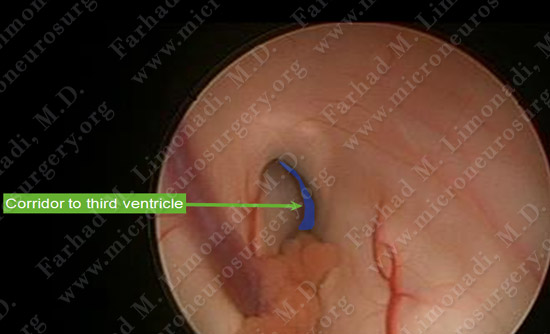
The corridor for entry to the third ventricle through the foramen of Monro to perform third ventriculostomy is very narrow!
As then neuro-endoscope is carefully driven closer to the forman of Monro, the colloid cyst becomes readily visible. The Neuro-endoscope is gently driven through this narrow corridor into the third ventricle.
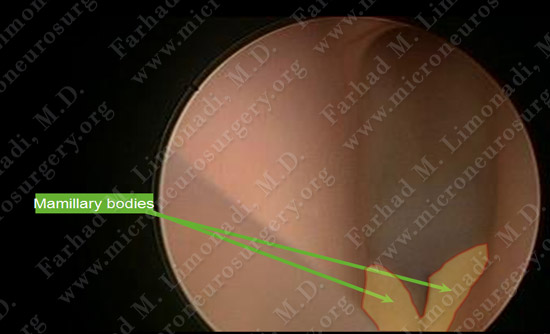
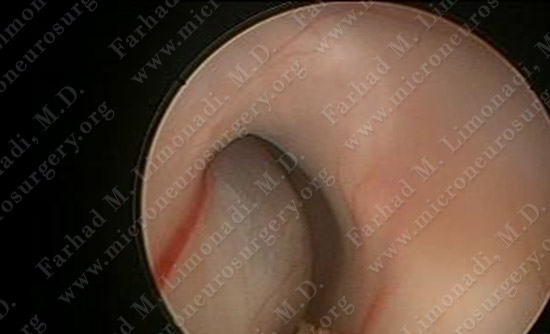
Upon entry to the third ventricle, the very narrow space is carefully inspected with landmarks identified.

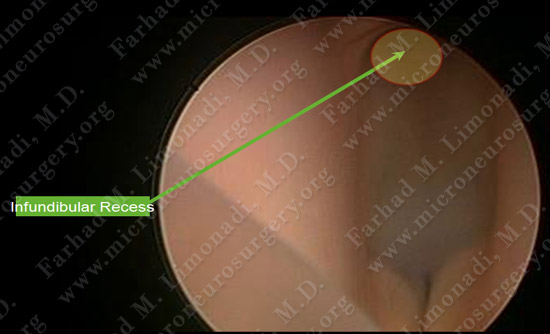
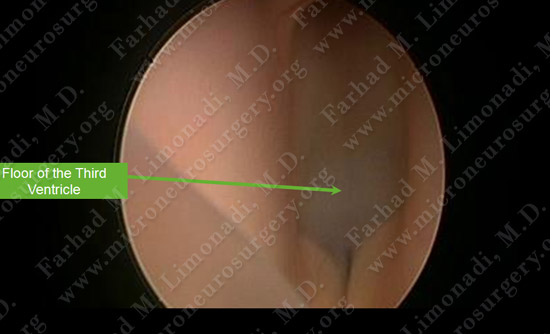
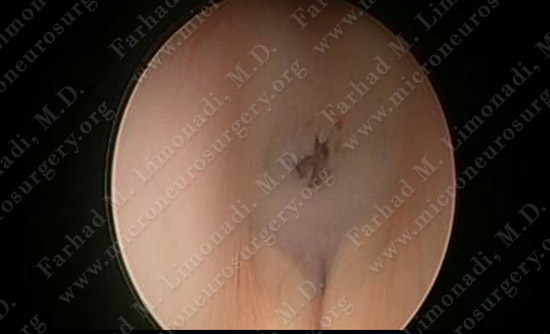
Third ventriculostomy is performed as the first step by creating a stoma, connecting the third ventricle to the perimesencephalic cistern.
Neuro-endoscope is then carefully utilized to remove the colloid cyst. A septum pellucidotomy allows entry to both frontal horns of the lateral ventricles with dissection of the cyst from both Foramen of Monro.

Tumor/Cyst Specimen which was sent for pathological review
Post-op Imaging
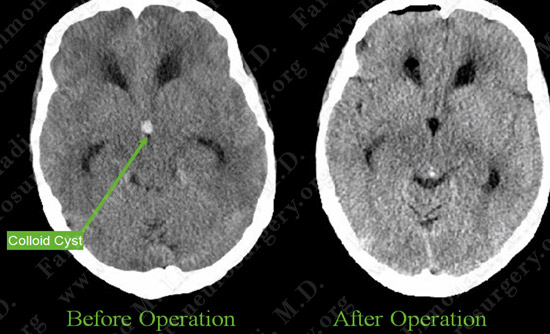
Post op MRI shows complete resection of the tumor with no injury to surrounding neuro-vascular structures. Most importantly patient had no neurological deficit after the operation.
Post-op Course
- She was discharged from the hospital shortly and returned to full function and employment.