













Case Presentation:
Acoustic Neuroma - Case 6
History & Physical
- 71-year-old gentleman with known acoustic neuroma diagnosis which after a period of observation was discovered to be growing in size. He underwent stereotactic radiosurgery (radiation treatment); however, despite this, his tumor continued to grow in size. He was complaining of facial paralysis, numbness, difficulty with swallowing food, and loss of gait and balance.
- On physical examination, he exhibited significant left facial weakness (House-Brackmann grade III-IV as the result of cranial nerve 7 injury), was deaf and had a difficult time with gait and balance (cranial 8 injury), left facial numbness (cranial nerve 5 injury), with dysphagia (cranial 9, and 10 injury), as well as with a tongue that protruded to the left (cranial 12th injury).
Imaging
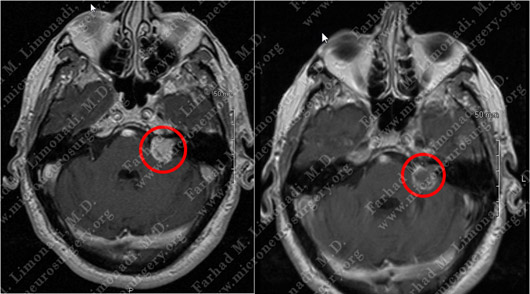
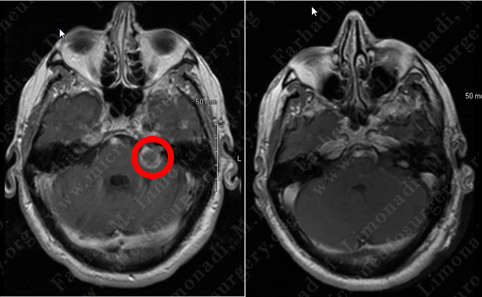
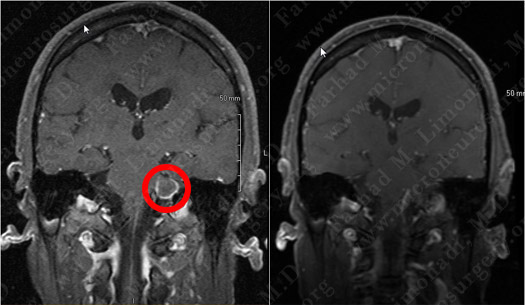
Before Radiosurgery After Radiosurgery
MRI scan of patient's brain before and after radiosurgery shows the tumor to have gone through central necrosis with peripheral enhancement.
Treatment
- He initially underwent treatment with steroids to help with edema and with the knowledge that this pattern of radiographic change and edema typically is followed by tumor shrinking in size.
- However, after nearly a month of steroid administration and continued surveillance, patient’s symptoms worsened and follow-up MRI showed progressive enlargement of the tumor and mass effect on the brain stem.
Surgical Procedure
- He subsequently underwent a left retrosigmoid craniectomy with surgical resection of this brain tumor using stereotaxy and brain mapping, intra-operative neurophysiological monitoring (including facial nerve monitoring), SSEP, MEP , and brain stem auditory evoked response (BAER).
- Tumor is removed in a gross total fashion from the cerebello-ontine angle as well as from the internal auditory canal. This tumor had scarred and was intimate with cranial nerves 5 and 7 and was impinging on cranial nerves 9, 10 and 12.

Computer Navigation
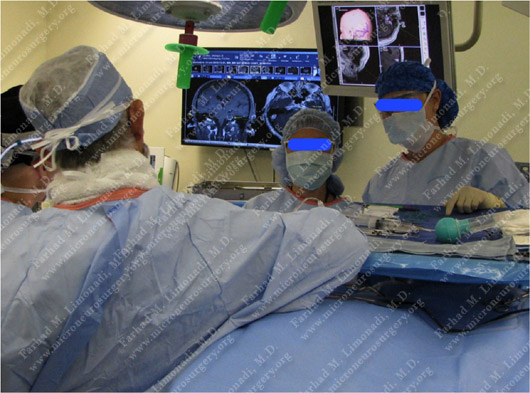
Computer navigation and mapping is utilized and reviewed during the operation.
Pathology
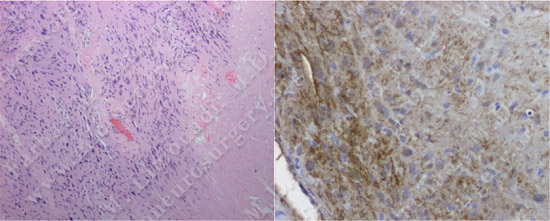
The pathology of the tumor confirmed the diagnosis of acoustic neuroma (vestibular schwannoma).
Post-op Imaging
Post-op MRI confirms complete resection of the tumor with no injury to surrounding neurovascular structures.
Post-op Course
- Postoperatively, the patient's facial weakness was unchanged, his facial sensation slightly improved, his swallowing difficulty improved; his gait and balance problem improve as well. He was discharged home in good health.