













Case Presentation:
Metastatic Lung Cancer to Brain - Case 14
- 60+ year-old man who presented with new onset of tonic-clonic seizure.
- He has been experiencing weakness of right lower extremity for a few weeks which had limited his mobility.
- On physical examination he had profound weakness of upper and lower extremities on the right side.
- Further work-up including CT of chest, abdomen, and pelvis demonstrated a mass in the pulmonary area (lung).
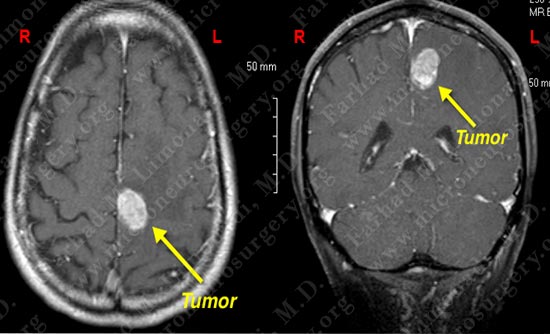
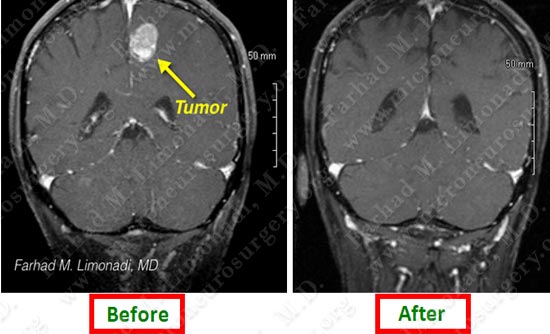
MRI scan of his brain shows a left fronto-temporal contrast enhancing mass (tumor). The tumor is marked in the right side of the slides (left side of patient's brain).
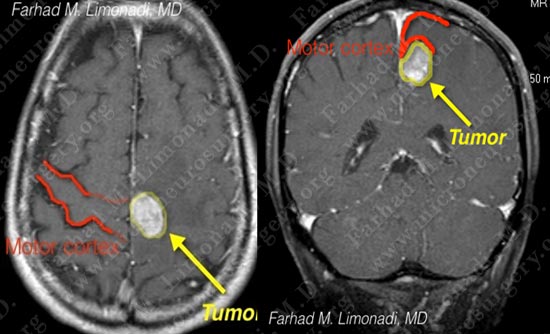
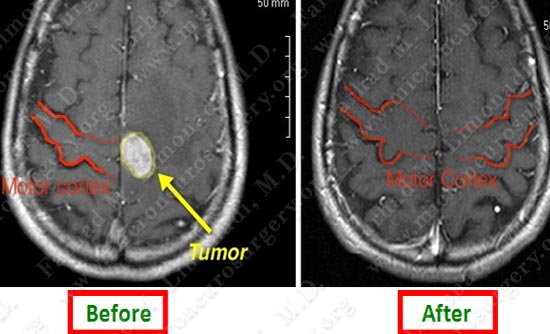
The tumor is pressing and has distorted the motor cortex (left slide: the opposite side motor cortex is marked). On the coronal view (right slide) the tumor is buried underneath motor cortex. These attributes make surgical removal of the tumor without injuring the motor cortex technically difficult.
Treatment Plan
- Patient was indicated for surgical resection of the tumor.
- He underwent left fronto-parietal craniotomy utilizing computer navigation, stereotaxy, and intra-operative electrophysiological monitoring.
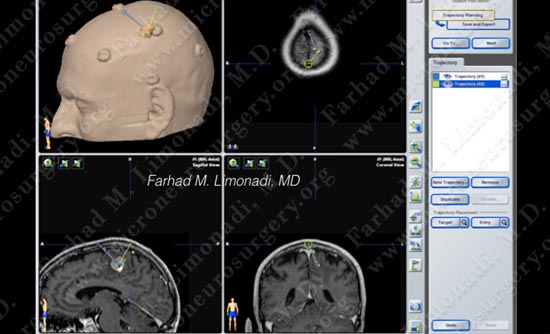
Computer navigation/ stereotaxy was utilized to locate the tumor with pinpoint accuracy and its borders with surrounding structures were studied using 3D modeling.
Surgical Procedure (view through the surgical microscope)
- A small bone flap of approximately 4 cm has been elevated, dura opened to the border of superior sagittal sinus.

Exposed brain is gently mobilized away from falx cerebri to expose the superior pole of the tumor.
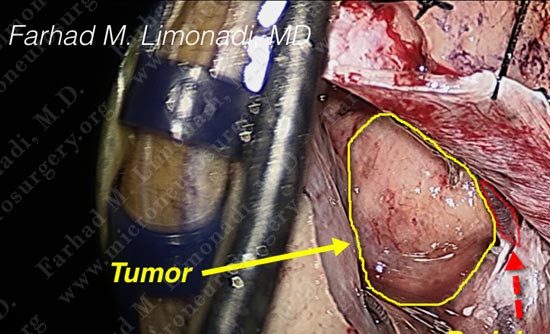
Superior pole of the tumor is nicely exposed. Draining vein which drains the motor strip is mobilized and preserved to avoid venous infarction.

Scale shows the size of exposure in centimeters.
Pathology

Tumor removed in one piece.
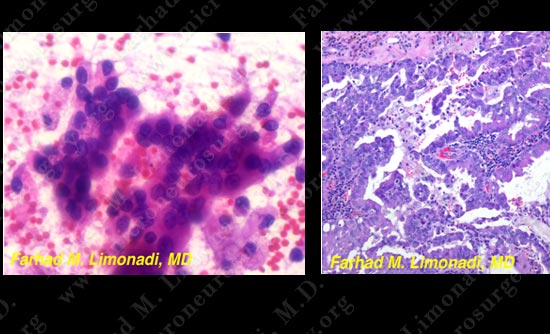
Pathology of the tumor was that of a metastatic adenocarcinoma. The diagnosis of metastatic lung cancer was established.
Post-op Imaging
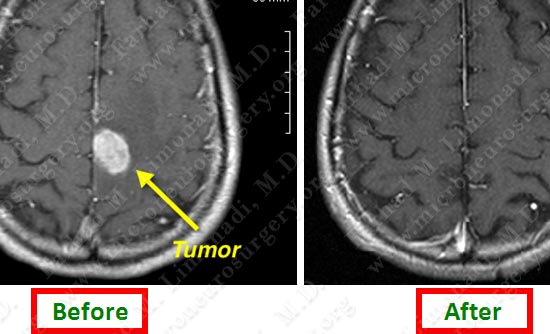
Post operative MRI shows complete resection of tumor with motor cortex unharmed and returned to its normal morphology.
Post operative MRI shows complete resection of tumor with motor cortex unharmed and returned to its normal morphology.
Post operative MRI shows complete resection of tumor with motor cortex unharmed and returned to its normal morphology.
Post-op Clinical
- Patient did well post-operatively with motor function returned to normal. His lung cancer was surgically removed.
- In four weeks he underwent stereotactic radiosurgery (SRS) and chemotherapy for adjuvant treatment of the tumor and he remained tumor free.
The tumor is pressing and has distorted the motor cortex (left slide: the opposite side motor cortex is marked). On the coronal view (right slide) the tumor is buried underneath motor cortex. These attributes make surgical removal of the tumor without injuring the motor cortex technically difficult.